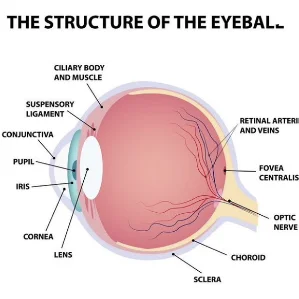
Retinopathy of Prematurity (ROP) is a disorder of the developing retina of low birth weight preterm infants, which potentially leads to blindness in a small but significant percentage of those infants. In full-term infants, the retina is fully developed, and ROP does not occur; however, in preterm infants, the development of the retina, which starts at the optic nerve head and proceeds anteriorly during the course of gestation, is incomplete. The extent of the immaturity of the retina depends mainly on the degree of prematurity at birth.
Neonatal Intensive Care Units (NICU) have set screening parameters that identify those infants at greatest risk, and baseline eye exams are performed by qualified ophthalmologists. Infants with a birth weight of less than 1,500 g or a gestational age of 32 weeks or less, as well as those at high risk for development of ROP, are screened. Upon examination, the findings are documented using a set nomenclature, which identifies the type of finding and location. Based on these findings, follow-up and/or need for laser treatment is determined.
The location of the vessels is defined by their distance from the optic nerve. Zone I encompasses the area of the retina, while the optic nerve acts as its center, visualized by a 28D lens. Zone II is the area of the retina consisting of the nasal periphery along with the optic nerve at its center. Zone III is the temporal crescent of retina in the periphery.
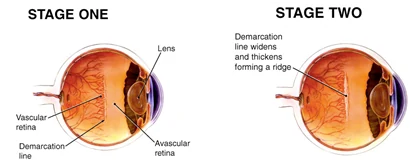
Most infants have immature blood vessels that can be classified as Stage 0. Stage 1 refers to when it becomes evident that there is a distinct line between avascular (no blood vessels) and vascular retina. Stage 2 occurs when the line of Stage 1 has become a ridge of tissue.
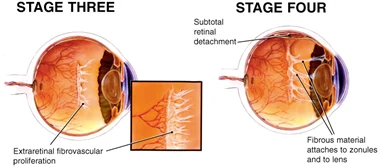
As the ridge begins to grow fibrous tissue on it as well as abnormal blood vessels, then Stage 3 has started. Stage 4 is defined by when the retina begins to detach due to anterior traction from the ridge of blood vessels. If there is only a peripheral traction retinal detachment, then it is Stage 4A. Stage 4B has macular involvement in the tractional retinal detachment. Stage 5 occurs if the entire retina is detached.
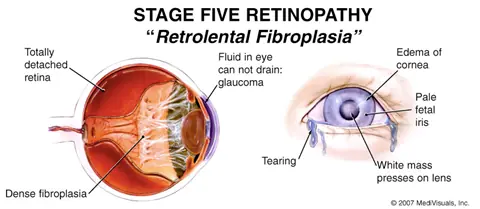
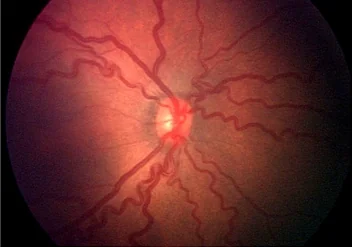
The character and appearance of the blood vessels near the optic nerve helps to define a characteristic known as Plus Disease. An infant with Plus Disease has very tortuous and engorged blood vessels. The presence of both Plus Disease and extensive Stage 3 Disease warrants early ablative laser to the avascular retina. If the ROP has already progressed to Stage 4 or 5, then only surgical intervention is possible. Surgery for ROP is wrought with technical difficulties and Stage 5 Disease almost always results in blindness. Poor visual outcomes are possible despite possessing good surgical skills.
 In developed countries, NICU have strict criteria for oxygenation and nutrition, which has led to less premature infants requiring laser and surgery. Strict screening guidelines are essential to identify at-risk infants and have them screened in a timely fashion. Due to the medico legal environment, the number of qualified ophthalmologists willing to perform screenings is continually declining. The lack of availability of qualified ophthalmologists in some areas of the country has led to telemedicine opportunities using equipment such as RetCam, a contact retinal photographic digital camera whose images can be transmitted via the Internet to a geographically distant reading center.
In developed countries, NICU have strict criteria for oxygenation and nutrition, which has led to less premature infants requiring laser and surgery. Strict screening guidelines are essential to identify at-risk infants and have them screened in a timely fashion. Due to the medico legal environment, the number of qualified ophthalmologists willing to perform screenings is continually declining. The lack of availability of qualified ophthalmologists in some areas of the country has led to telemedicine opportunities using equipment such as RetCam, a contact retinal photographic digital camera whose images can be transmitted via the Internet to a geographically distant reading center.
ROP is a sight-threatening disease, which advances in a progressive fashion. Some diseases can be very aggressive, especially in extreme prematurity (24 to 26 week old premature infants). Posterior Plus Stage 3 ROP Disease complicated with poor dilation and anterior vascularity may require treatment with Anti-VEGF agents such as Intravitreal Avastin when ablative laser would result in laser to the macula or the view is not sufficient to attempt laser. Modern NICU have strict criteria to identify at-risk infants, and adherence to policies is imperative to keep the infants from falling through the cracks. Education of the parents stressing the importance of outpatient follow-up and the timeliness of appointments is key. Delaying a week or two can result in missing the small window of opportunity in which treatment is possible. Any delayed care by the parent might result in irreversible blindness.

Education of the parent is not only important for ROP but also for the other eye conditions that can occur in premature infants. Babies who are born prematurely are at increased risk of needing glasses at an early age (usually myopia-near sighted). They also tend to prefer one eye to the other and can result in a lazy eye (amblyopia), which will require patching at an early age. Also, they tend to have a wandering eye (strabismus) and may need surgery to enhance the potential for binocular vision. It is recommended that all premature infants see an ophthalmologist that specializes in children’s vision by 4 to 6 months corrected gestational age.
Prematurity can affect the eye by causing ROP, strabismus, myopia or amblyopia. All of these conditions can be treated effectively if identified and treated in a timely fashion. It is imperative that the NICU personnel instruct and educate the parents to the lifelong eye care that will be needed. It is also important to realize that these parents can be overwhelmed by the quantity of doctors’ visits needed by their premature infant, but the importance of their eye exams should be stressed and documented.

Contact Retina Specialty Institute
Inherited retinal diseases require the treatment of a highly experienced specialist. At Retina Specialty Institute, our practice is dedicated to the treatment of all forms of retinal diseases and disorders. Our experts have deep experience in the diagnosis and management of inherited retinal diseases.
The doctors at Retina Specialty Institute have either authored or reviewed and approved this content.
Page Updated: